In this video we’re going to talk about bone spurs causing tailbone pain or coccyx pain.
This is the next in my series of videos going chapter by chapter through my book “Tailbone Pain Relief Now!” to share some of the information that’s in each chapter.
To do that in a video format that’s available online as it is here allows us to interact more because you can post comments or questions or your stories down below this video.
So this now is Chapter 9 within my book.
So Chapter 9 is Bone Spurs Causing Tailbone Pain.
So what we’ll cover in this video is what is a bone spur, how does it happen, what is it made of, where is it located within the coccyx and how does it cause pain.
We’ll talk about a few other aspects as well.
So first of all what is a bone spur?
A bone spur is when there’s a little bit of additional bony material beyond the normal amount.
One thing I compare this to sometimes is: if you think about when you get calluses on your hands or feet. There’s thickening of the skin that causes a callus of the skin.
Well, similarly there can be thickening of the bone causing a callus of the bone and when that callus is located in a particular way that it forms a point that is called a bone spur.
Or some of my colleagues in Europe often will refer to it as a bone spicule.
It’s the same thing.
So if I show you here an illustration from the book probably will do a good job of showing you what we’re talking about here.
So basically this is a side view of the coccyx or tailbone.
So if we looked at the coccyx like the sacrum and coccyx like this normally you can see how the tailbone curves forward into the pelvis.
But now in this case it starts curving forward.
But you can see here down on the lower end there’s a little bit of extra bone.
I’ve highlighted in yellow here on the illustration just to make it more clear where there’s a little bit of extra bony material there.
That is a bone spur or a bone spicule.
And it’s often relatively small.
So you could say maybe smaller than the size of a pea or a pebble.
But it can cause a lot of pain.
Just like the same way that a small pebble within your shoe would be very, very painful if you were walking on that all day.
Every time you put your body weight on it you would obviously have a lot of pain in your foot after a while from doing that.
And similarly when you have a bone spur the size of a pebble down here at the lower tip of the coccyx that can cause a lot of pain as well.
Because every time that you go to sit down basically you’re sitting… if this is… I’ll have the book represent the chair.
Here you go to sit and now you’re going to be pinching the skin in between the bone spur and the chair that you’re sitting on.
And especially if you sit leaning partway back you’re really going to be poking that bone spur down on the skin and down towards the chair.
So the bone spur itself is made of bone.
It is bone just like the callus that you have on your hands or feet is made of skin.
It is skin.
So a bone spur is made of bone.
It’s a thickening of the bone that forms a focal point.
And where does it occur at the tailbone the vast majority of the time?
It is located down at the lowest tip of a tailbone.
So the lowest tip of the coccyx is the spot where you see the bone spur most commonly.
And the other question that comes up is well… what direction… if it’s coming to a point, what direction is that pointing typically?
It’s pointing behind you.
So it’s pointing backwards.
So back to our anatomic model here again…
This would be a model of the sacrum and down here is the coccyx.
You can see the whole thing is curving forward.
But if there was a bone spur it would be pointing back the other way.
The bone spur would be pointing back that way, the way that the pen is showing here.
So that’s a little bit about what the bone spur is made of, and where it’s located, and the direction that it points, and the way that it causes pain especially when you’re tilted leaning back.
But even with sitting upright it can often be very painful as well.
The things that are done to treat the bone spur we’re going to talk about in some of the later videos when we’re talking about treatments of various types of tailbone pain.
The book is sort of divided so that the first half of the book is about the diagnosis and what it is that causes tailbone pain, and goes through a variety of different causes.
And it’s super important that prior to starting treatment that you actually have a sense of what it is that’s causing your tailbone pain in the first place.
How is that assessment made when we’re looking at bone spurs? There’s two or three main ways.
Number one of course is listening to the patient’s symptoms.
They have pain at the coccyx.
Right in that area.
Pain with sitting, pain with sitting leaning part way back.
Sometimes they may have some pain during transitions from sitting to standing but those things are true about most causes of tailbone pain.
The ways that you would distinguish that the bone spur specifically would be… Number one, on physical examination if the physician is careful while they are touching even just pressing externally along the back of the sacrum and the back of the coccyx if there was a spur right here where my finger is you may be able to feel that projection coming backwards.
It’s almost pointing if this patient was laying on the table here and they’re facing down towards the floor or the table their back is pointing up towards the ceiling.
And in this example the bone spur would be here pointing somewhat up towards the ceiling.
And just from a careful physical exam just gently pressing along the back wall of the sacrum and coccyx you can kind of walk your finger down and and you can sometimes feel the spur pointing upwards.
So another way you can assess for that is by getting imaging studies.
Most commonly that’s done by x-rays or radiographs.
And it’s important that they do the side view and not the front view because the side view will show you that silhouette that will show if there is a bone spur sort of sticking out.
And we’ll talk more in another video covering another chapter about the different tests that are done for tailbone pain.
You can see it on x-rays, MRI CT scans, etc but only if any of those tests are done properly.
Unfortunately a large percentage of the time the imaging studies are NOT done properly.
So that’s a general scoop about bone spurs causing tailbone pain.
Obviously there’s a lot more information within that chapter within the book.
But I wanted this video to provide us an opportunity to generally cover the topic.
And also for you to post your comments down below.
Comments or questions or thoughts.
Or if you’ve had a bone spur someplace else… at your shoulder or sometimes people get them on the sole of their foot with plantar fasciitis.
It’s the same idea that that bone spur, that pointy projection of bone, starts to pinch things.
So if it’s your shoulder it pinches into the rotator cuff muscles when you try to reach up overhead.
At the sole of the foot it pinches the skin when you take that first step in the morning and press down.
It can pinch the soft tissue structures on the sole of the foot.
So that’s a little bit about bone spurs.
Post your comments down below and if you’re interested in getting the the book itself the easiest way to get that is to go to the website www.TailboneBook.com.
It is available on Amazon, but if you go to www.TailboneBook.com it will give you the direct link for the Amazon site for your country.
Whether you’re getting the e-book (which is available worldwide you do not need an e-book reader. You can just read it online.)
So anyplace that has internet access you can get the e-book and also the paper copy.
I’m In My Bookshelf! Making Tailbone Pain Videos. 🙂
This is very break from my series of coccyx pain videos that have been giving you highlights from the chapters of Dr. Foye’s book, “Tailbone Pain Relief Now!”
In this video, I show you how I make the educational videos that I have been posting online.
Summary: My very basic, no-frills set-up is usually just propping up my iPhone to show me and the educational props I have on my bookshelf. I usually do not edit the videos after I record them. It does then take some time to upload them, label them, create captions (for hearing impaired people), etc.
The actual VIDEO is at the bottom of this page.
Here is the TEXT from the video:
Hi. I’m Dr. Patrick Foye, M.D., Director of the Coccyx Pain Center or Tailbone Pain Center, online at www.TailboneDoctor.com.
And in one of my videos in the comments down below the video, somebody was asking me where I was doing these videos because it looked like there was this weird low ceiling, or something along those lines. So I thought I would show you just very briefly where I am doing these videos lately.
I am basically doing these videos inside a shelf on my bookcase. It turns out to be a pretty easy way for me to do it. I have a shelf that is mostly empty except for a lot of educational stuff that I have: a coffee mug that looks like a part of the vertebral spine and I have my plastic model of the pelvis including of course the sacrum and coccyx and I have other versions of the coccyx that move around a little so if I need to demonstrate that in some of the videos.
And basically I have been setting the camera up here so I can put up whatever is the chapter in my book that I am covering in that video and I will choose some kind of a colored paper background just mainly so that I can see the borders and at a glance I can see from the different videos that from the color and from the title it will remind me which video is which so that I can keep them straight when I am uploading them.
And then down here on the next shelf I have got some images printed out from my book so that if I am talking about a fracture and I need to show a fracture or I need to show a dislocation, or I need to show the coccyx and the spine in general, etc, that I have those things on hand as I am making these videos in my bookshelf.
So anyway, if you were wondering, maybe you are not, but if you were, that is what I am doing lately as a way to try to keep creating these videos, because a lot of people seem to find them helpful for providing educational content for the topics related to the tailbone and lately going chapter by chapter through my book, “Tailbone Pain Relief Now!”
So anyway, I thought you might be interested if you have been watching the videos and wondering where I was or what this was, now you know.
This video is about tailbone dislocations. This video is the next in my series of videos going chapter by chapter through my book, “Tailbone Pain Relief Now!”
The idea of the videos is to give you some sense of what is covered in each of the individual chapters. And also in this format to provide a way for us to interact about the topics.
So you can post comments and questions and your experiences down below this video if you have things to say about tailbone dislocations, coccyx dislocations.
This is Chapter 8 within my book. and the most important thing with tailbone dislocations often is to distinguish a dislocation from a fracture and these are very very different.
And if you think about it, a tailbone dislocation is when one bone is no longer lined up and attached to the next bone. So I will show you that here.
Here is an image from my book. This would be showing a partial dislocation where this bone is no longer lined up with the bone beneath it. It is almost a complete dislocation in this illustration here.
But, the thing I will call your attention to is that each of the individual bony segments is intact. none of those are broken. So that is very different than a FRACTURE where there is a CRACK in the bone or a CHIP off the bone.
In this example with a DISLOCATION, by contrast here, there is NO chip in the bone. There is NO crack in the bone. Each individual bony segment is INTACT. So it is NOT a FRACTURE. This IS a DISLOCATION. It is very very common that I see this mistake (mixing up coccyx fractures and coccyx dislocations) made by emergency room physicians or primary care doctors or even by musculoskeletal physicians or radiologists who should know better and would know better in other parts of the body.
But what they will do is they will see this separation here between one bone and the next. And because they think of the tailbone as being a singular bone rather than a series of bones, they will think, “Oh, well this segment must have fractured off that one above.”
But that is NOT how we you make a diagnosis of a fracture versus a dislocation. We look to see IS THE INDIVIDUAL BONE ITSELF INTACT?
And that becomes important because it is important in terms of having an accurate diagnosis first so that then you can decide what you need to do or don’t need to do in terms of your treatment options.
So the way that you diagnose a dislocation at the tailbone is typically after your history and your physical examination is imaging studies. Often x-rays will be able to make this determination, especially if you can get sitting-versus-standing x-rays. Because there are times where the patient will have something that looks normal in one position, but when they are sitting (which is their painful position) they may have a dislocation that only appears while they are sitting. That is called dynamic instability, which is one of the other chapters in the book which I have covered in another video as well.
So the idea about the dislocations is that you want to make an accurate diagnosis. And you want to know exactly what joint is dislocating.
So that if treatments are being provided in the form of injections or things of that nature then the physician should know where to target any such procedure or any such injection.
Or in severe severe cases of a small percentage of the time that need surgery, then the surgeon needs to make sure that he or she has taken care of the area where you are actually having the dislocation.
So that becomes really important.
Again, dislocations can be very common at the tailbone.
They can be very challenging to treat.
And you need the proper imaging studies in order to make the diagnosis in the first place. If the proper imaging studies are NOT done, then often the patient, unfortunately, is told, “Everything was normal, everything looked fine, there is nothing wrong with your tailbone.” When really you have a dislocation or some other injury or problem.
What is it that causes the dislocation? Well, basically it is a problem with the LIGAMENTS. Normally, ligaments are what hold one bony segment to the next. Whether that is here in my fingers or in the bones of the coccyx, the ligaments span from one bone to the next bone. And if those ligaments are stretched or torn, then you no longer have that stable connection holding one bone to the next. And then the bones will shift or move which is, again by definition, a dislocation.
There is a lot more in the book in terms of the appropriate tests to get and the whole second half of the book is about different treatment options. But hopefully you have a sense now at least of how to distinguish a dislocation from a fracture and understand what a dislocation is. And also understand that some dislocations only show up on the x-rays while you are actually sitting and putting your body weight onto it, which is why it is important to have the sitting or seated x-rays performed.
I hope that information is helpful for you. If you are looking for a copy of the full book, the easiest way to get that is to go to www.TailboneBook.com. And on there I have the links to all the different Amazon pages for whatever country you may be in.
You can get the paperback copy. It is 272 pages.
Or you can get the electronic copy of the book, the e-book, which you can download that worldwide, any place where you have an internet access, you can get the book that way if that works best for you.
So, post your comments down below. I will be interested to read those and see your thoughts or comments. If you have been told you had a dislocation but they never did the imaging studies, which would be crazy, or if you were told you did not have a dislocation but the imaging studies showed you actually did, or they never did the proper tests or what have you, post your comments or questions down below.
If you are looking to find me online or to come for an evaluation here at the Coccyx Pain Center, the easiest way to find me is to just go to my website which is www.TailboneDoctor.com
Okay. Bye bye now.
Here is the actual VIDEO:
Here is the screenshot thumbnail image for the video:
Chapter 8 of Tailbone Pain Book: Coccyx DISLOCATIONS, DISLOCATED Coccyx
Severe Tailbone Dislocation on coccyx X-ray, causing coccyx pain, tailbone pain, coccydynia
To get your copy of the book “Tailbone Pain Relief Now!” go to: www.TailboneBook.com
For more information on coccyx pain, or to be evaluated at Dr. Foye’s Tailbone Pain Center in the United States, go to: www.TailboneDoctor.com
The electronic book is now published containing all of the papers written by those who lectured at The First International Symposium on Coccyx Disorders, which was in Paris in 2016.
The book is available for purchase in e-book format only. (Currently it can be purchased and read on an iPad or on an android tablet. Currently it can not be downloaded onto a regular laptop or desktop computer nor onto an iPhone, but those options may be available in the future.)
Here is the link: https://www.bestpractice-publishing.com/index.php/product/coccyx-disorders/
Here is the cover, which I think looks beautiful:
Coccyx Book Cover, from Paris 2016 Symposium
Here is the first page of Dr. Foye’s chapter on Ganglion Impar (Walther) Sympathetic Nerve Procedures for Coccydynia.
Ganglion Impar Chapter by Dr Foye, from Coccyx Book from Paris Symposium 2016, Just Page 1
Here is the citation for referencing this chapter:
Foye, PM, Shenouda M. In: Maigne J-Y, Doursounian L. (ed.) Coccyx Disorders. (Best Practice Publishing, 2018). Papers from The First International Symposium on Coccyx Disorders. Chapter: Ganglion Impar (Walther) Sympathetic Nerve Procedures for Coccydynia. Pages 106-116. Online at: https://www.bestpractice-publishing.com/index.php/product/coccyx-disorders/
This is the next in a series of coccyx pain videos, giving you highlights from the chapters of Dr. Foye’s book, “Tailbone Pain Relief Now!”
The actual VIDEO is at the bottom of this page.
Here is the TEXT from the video:
Hi, I’m Dr. Patrick Foye. I’m an M.D. or Medical Doctor and I’m the Director of the Coccyx Pain Center, or Tailbone Pain Center, here in the United States. I’m online at www.TailboneDoctor.com.
And this is the next in the series of videos going chapter by chapter through my book “Tailbone Pain Relief Now!”
And in this chapter, we are up to chapter number 7, which is Tailbone Fractures: The Broken Coccyx. And this is a really important chapter because: fractures of the tailbone, number 1, they can be very painful and they can take a very long time to heal; and number 2 is that it is probably the most over-diagnosed and misdiagnosed condition at the tailbone.
It is very very common that people will have some trauma, they slip and fall, they land on their buttocks. They land on their coccyx or tailbone. And then they have some pain. And maybe they go to see their primary care doctor or a musculoskeletal specialist or they even go to the emergency room.
And the doctor will say, “Well, you know what? You fractured your tailbone.” Sometimes without even getting an x-ray. Or, they will get the wrong x-ray. It will be of the lumbar spine or they won’t do the proper imaging to properly show the tailbone. But they will be told, “You know what? You probably fractured your tailbone.”
And it is important because you really want to have an accurate diagnosis so that you can develop a treatment plan based on an accurate diagnosis rather than just somebody saying off the top of their head, “Maybe it’s fractured.”
The way I would think about this and the way I describe it to patients is as follows: If you think about the bones of the coccyx, really they are… this is the sacrum up here and then the coccyx or tailbone is shown right down here. And from the side view it looks sort of like that.
So the coccyx is really a series of bones. You can see that there’s a number of bony segments here. And sometimes parts of them are fused together and sometimes not. And the reason that is important in this chapter and this discussion about fractures is that sometimes an emergency room physician or maybe even a radiologist will look and see that there’s discrete individual segments at the tailbone as shown here. And they will think, “Oh well, you know what? Maybe that section down at the bottom is fractured off. I see a space, I see a lucency, a clear area where there’s no bone there.”
And the reason why that can be misleading is because there is supposed to be a clear space between the bones if the bones are not fused together. Just like if you took an x-ray of my fingers, you would have a bone here and then you would have a clear space where the joint is, and then you would have the next bone and a space, and then the next bone and a space. So where the knuckles are, there would be a joint space in those areas.
And the same is true at the tailbone. But unfortunately, many many times the emergency room doctor or the radiologist will somehow forget the basics that they know anywhere else in the body. And when it comes to the tailbone, they will see that lucency and they will call it as a fracture. They will see that lucency and they will say, “Yes, there’s a chip of the bone that came off”, when really it is just the normal joint space that we expect to be there in most of us (in all of us that do not have a “fused” coccyx).
So, what is a fracture then? Well, a fracture is when you actually have broken the bone. And the easiest way to think about this is, I describe it as if you think about a stack of bricks, if you were stacking bricks one on top of the other, the tall way, that would be a little bit similar to the bones in the coccyx stacked one on top of the other here.
And you would expect there to be a joint space, a little bit of space in between those bricks, a little sliver of air in between brick number 1 and brick number 2 and brick number 3, etc. And when you see that little bit of joint space, that is NOT a fracture. The brick, each individual brick, if it is still intact then there is NO fracture.
So similarly for the coccyx, if each individual bone of the coccyx is intact, there is NO fracture. Now what people may have is they may have a DISLOCATION, they may have where one bone has moved away from the other, but that is NOT a fracture. Back to our brick example, that would be two bricks that are moved apart but they are still intact, each individual brick is not chipped or broken.
So that’s a real distinguishing factor between a dislocation and a fracture. And there is another chapter where we will talk more about dislocations.
So then, what is a fracture? Again, a fracture is when piece of the bone is actually broken; so as shown here, that can happen in a number of different ways. In this top bone here we have basically what is called a “hairline fracture”, which is you can see the fracture line sort of going through the bone here, but the pieces of the bone are still essentially together. So that’s a hairline fracture.
And what is more severe is what is called the “displaced fracture”, which is here where a piece of the bone has actually separated from the rest of the bone. So, the difference between a hairline fracture, also called a non-displaced fracture and a displaced fracture is whether one piece of a given bone has actually separated from the other piece of that same bone that it was normally attached to. So that’s a non-displaced fracture versus a displaced fracture.
Another term you will sometimes hear is a “comminuted fracture”, which just basically means that unfortunately the bone is shattered so it is broken up into many many pieces. So think about dropping a teacup and it shatters into many pieces that would be equivalent to a comminuted fracture.
So there are again different types of fractures. And in the chapter we go into the fact that to make a diagnosis of a fracture you really need imaging studies; so just knowing that somebody is tender there or that they have some bruising or that they had some trauma, that alone is not enough to officially make a diagnosis of a fracture. You really need to have the imaging studies to see what is going on with the bones and are the individual bones intact or not.
So, to do that you have to have the proper imaging studies done and unfortunately, it is very very common that the proper imaging studies either are… no imaging are done at all, or the proper imaging studies are not performed. So the ordering physician and the radiology technician and the radiologist need to have some insight or experience in evaluating tailbone pain and tailbone problems and tailbone injuries in order to do the proper tests.
The treatment for a fracture really depends on how severe the pain is and there are medications, and the book goes into more of the details, but there are medications that can be used to help to relieve the pain. But a couple of things that I will point out is that treating a fracture at the tailbone is very different than treating a fracture in most other parts of the body.
Because if I had a fracture in my arm, what we could do is we could put my arm in a cast. But you can’t put your tailbone in a cast. For my arm we could put rods and screws in place to hold the fracture stable. But really that’s not so easy at the tailbone. The tailbone are these little tiny bony segments and putting rods and screws through them off the tailbone bones themselves would probably crumble to some extent, so it is really challenging.
Also, you don’t want to just fuse it with rods and screws because then you would be sitting on rods and screws which would be painful and also there is supposed to be some mobility or movement at the tailbone, so if you were to fuse it with orthopedic hardware, you would lose the normal mobility that you need and then the tailbone would be in the way, every time that you go to sit down it would fail to move out of the way. It would fail to move as normal.
So also you can do non-weight-bearing in other parts of the body, like if I had a fracture in my leg we could use crutches so I don’t put any weight on that leg. But at the tailbone that is not so easy. At the tailbone you are basically saying, well do not sit, because that is the weight-bearing position.
But it is very very difficult in modern society to go through the day without sitting; you need to sit to drive in your car or to commute or while you are on your computer workstation to some extent. And some of that we can work around, but still we can stand more, but it is very very difficult to stand through the entire day.
So, very very challenging in some ways in terms of treating fractures at the coccyx. There certainly are treatments that can be done. Later in the book we will get into the chapters about treatment, but there are medications, there are injections, there are other things that are available that do provide relief for the majority of patients.
So there is more information in the book, if you are interested in getting a copy of the book, the easiest way to do that is to go to www.TailboneBook.com. And from there I will have the links to specifically to the direct Amazon pages for your specific country whether you are in the United States or Canada or Europe, U.K., etc. I have those listed on there.
So that is the easiest way to go to get the book. The book is available both as a paperback copy and also as an e-book, so you can get the e-book copy which you can basically download and read that anyplace in the world where you have internet access. You can get that book that way.
If you are looking to find me online, the best way to find me is to just go to my website which is www.TailboneDoctor.com and you can find me there.
Post your comments down below. If you have questions about fractures at the tailbone. If you have been told you had a fracture but they never did an x-ray or imaging study to actually confirm it. Or you had a fracture but you found out later it was never fractured in the first place. Or you were told that it wasn’t fractured and finally they got the imaging and found out that it was. Post your comments and thoughts and questions down below and we will be on the lookout to respond to those.
I hope this video is helpful and all the best. Bye bye.
Here is the actual VIDEO:
Here is the screenshot thumbnail image for the video:
There are multiple reasons why some coccyx injections do not help to relieve coccyx pain (tailbone pain, coccydynia).
The physician doing the injection did not start by accurately diagnosing cause of the tailbone pain.
If the doctor has not tried to figure out exactly what is causing the pain, how would he/she understand the proper type of injection to do?
Also, how would the doctor know exactly where on the tailbone to do the injection?
For example, if there is one specific joint that is dislocating on the sitting-versus-standing x-rays, then it makes sense that the injection should target that specific joint.
Or, if the pain is being caused by a bone spur down at the lower tip of the coccyx, then it makes no sense for the physician to be focusing their injection up at the top of the coccyx.
This the MOST COMMON reason why injections do not help…. the doctor did not first make an accurate diagnosis.
I have seen this happen to countless patients who travel to see me to help figure out why the injections done by their local pain management doctors were not giving them relief.
The injection was done without imaging guidance (fluoroscopic guidance).
The bones and joints of the tailbone are small. That means that they are very small targets for injection.
Using fluoroscopic imaging during the injection helps the physician to more confidently know that the needle is placed at the correct location.
Injections done without imaging are sometimes referred to as “blind injections.”
Blind injections might be in the general area of pain. They may be nearby to the site of pain. But maybe not.
Regardless of whether someone gets great relief or no relief, it was a blind injection then neither the physician nor the patient is 100% sure about where the injection was done.
Lack of imaging guidance can also explain why sometimes the injections are helpful and sometimes they are not. Some of the injections may have placed the medication at the most helpful area. But other times the injections might have failed to place the medication at the best location.
The injection was not done at the coccyx.
This is crazy but true.
It is VERY common that a patient suffers from tailbone pain, but the treating physician is not very familiar with doing tailbone injections. So, the physician instead does a lumbar injection or a sacral injection, and “hopes” that this will somehow help the tailbone.
If possible, obtain a copy of your injection procedure note to specifically see whether you even received a coccyx injection. You may discover that the injection was a lumbar epidural, or a caudal epidural, or a sacroiliac injection. None of those are injections at the coccyx.
The pain is not coming from the coccyx.
If your pain is coming from someplace OTHER than your coccyx, then it is not surprising if an injection at the coccyx does not give relief.
For example, pain in the general coccyx area might be actually coming from the anus, rectum (large intestine), or a pilonidal cyst. Worse yet, the pain might be coming from a mass or cancer (malignancy). Cancers and other masses can start within the pelvis (such as prostate cancer, ovarian cancer, uterine cancer, cervical cancer, rectal/colon cancer, etc.).
The underlying coccyx problem has gotten worse, so that injections are no longer adequate treatment.
It is possible for underlying condition to worsen over time.
If the underlying condition is worsening, it made no longer respond as well to treatments that previously were very helpful.
Out of all these, the most common reason why coccyx injections fail to relieve coccyx pain is #1 above. The treating physician did not accurately diagnose the cause of the tailbone pain in the first place.
What are bone spurs and how do they cause coccyx pain (tailbone pain, coccydynia), foot pain, or shoulder pain?
Bone spurs: What Are They?
A bone spur is an area where there is thickening of the bone. It is made of bone. It is bone.
Just like your skin can become thickened skin and form a skin callous. Similarly, the bone can become thickened bone and form a spur.
On imaging studies, a bone spur often looks like an icicle hanging down from your rain gutter.
Bone spurs: Where Are They?
A bone spur can form on essentially any bone.
Some of the most common areas for bone spurs include:
Heel spur: this is a bone spur on the calcaneal bone on the sole of your foot. Is often seen in people who have plantar fasciitis. A classic symptom is if you have pain with walking. Especially common is pain on the sole of your foot when taking your 1st step in the morning.
Shoulder spur: this bone spur is sometimes called a subacromial bone spur. The bone spur presses or pinches into the rotator cuff muscles or tendons. With this, you would probably have pain with trying to reach overhead.
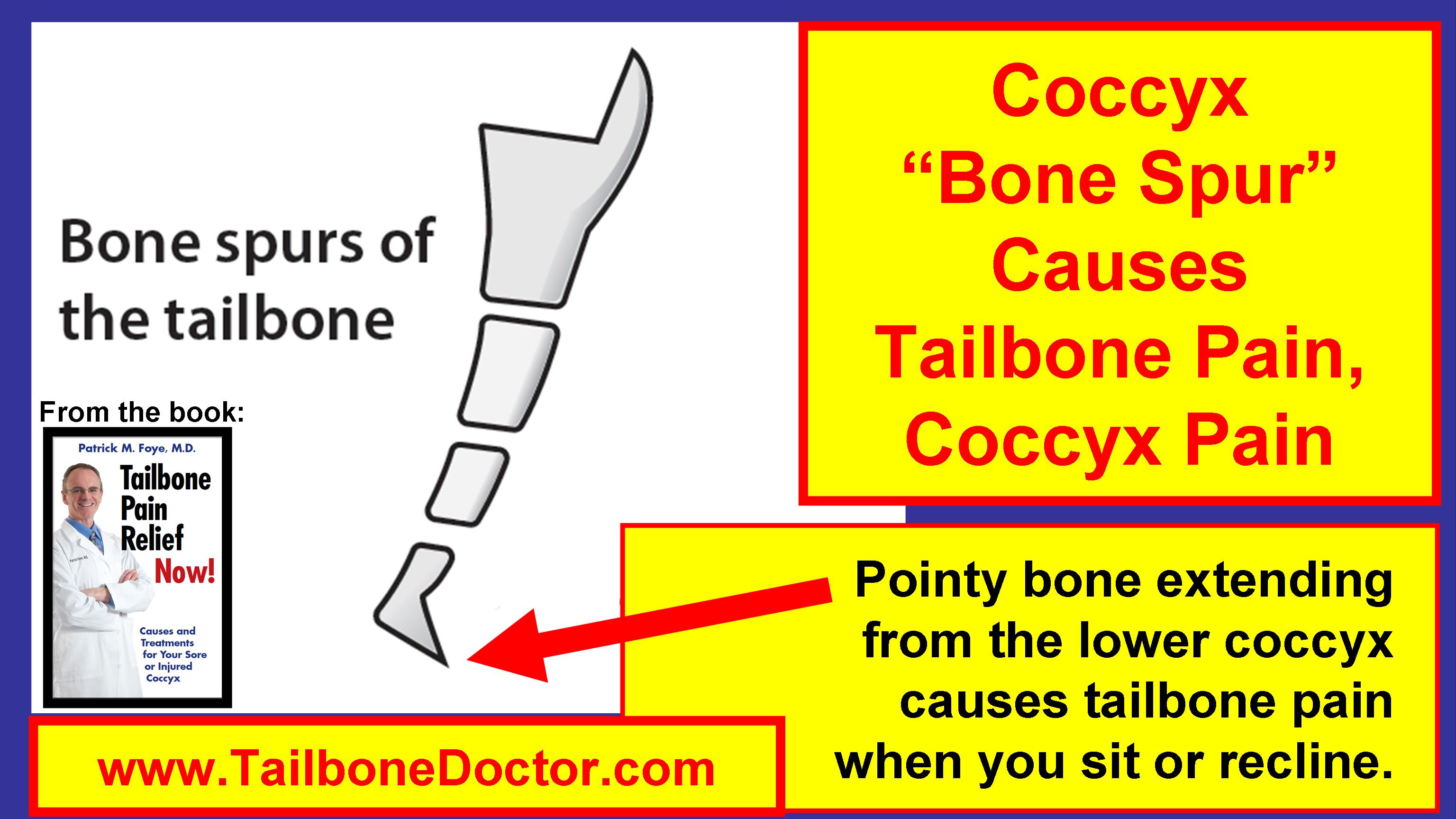
Coccyx bone spur: This is a bone spur on the lower tip of the coccyx (tailbone). When this happens, instead of the lower tip of the tailbone being rounded for words (like the bottom of her rocking chair), instead the bone spur points downward or backwards. If you have a bone spur on the lower tip of your tailbone, then sitting down causes the spur to pinch the skin in between the spur and the chair that you’re sitting on. Sitting leaning partway backwards (partially reclining) can be especially painful.
Do bone spurs in one part of the body increase your risk for bone spurs in other parts of your body?
I have had MANY patients over the years where I diagnose a coccygeal bone spur and as I am explaining it to them they respond by saying they already have a diagnosis of a plantar bone spur (plantar fasciitis).
It raises the question as to whether someone having bone spurs in one part of the body are more likely to also have bone spurs in another part of the body.
To my knowledge, there has never been a formal study to see whether bone spurs at the coccyx are also associated with bone spurs in other body regions.
But there may be some association, since the findings and symptoms are somewhat similar, just in a different location.
Coccyx Bone Spur Causes Tailbone Pain, Coccyx Pain, Bone Spicule
Apparently, in the United Kingdom, the National Health Service (NHS) has radiology protocols that explicitly deny the usefulness of tailbone x-rays (coccyx radiographs, xrays) for patients suffering with tailbone pain (coccyx pain, coccydynia).
A person in the UK who suffers from tailbone pain sent me the following link: (As of Feb-11-2018, this PDF can be downloaded using the Google Chrome browser, but not with the Firefox browser.)
Here are the relevant parts of the 220-page protocol, (the ALL-CAPS parts are theirs!) which specifically address coccyx pain:
RADIOGRAPHIC STANDARD
OPERATING PROTOCOLS
PRODUCED IN ACCORDANCE WITH THE ROYAL COLLEGE OF
RADIOLOGISTS GUIDELINES (2007) AND DEPARTMENT PROTOCOLS.
DEPARTMENT OF RADIOLOGY
STANDARD RADIOGRAPHIC PROJECTIONS
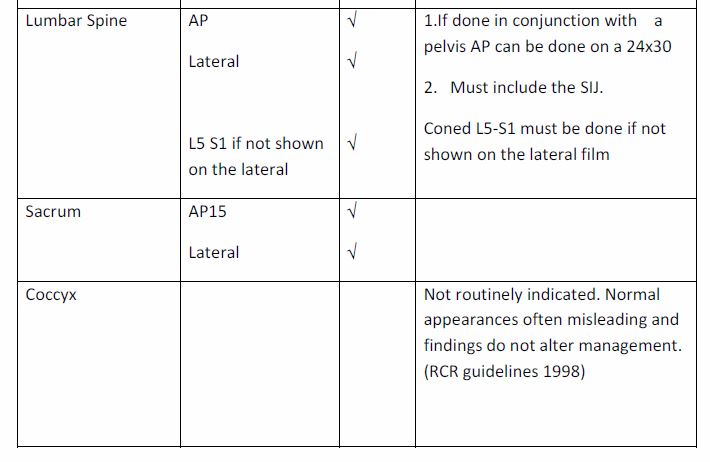
Page 14 of 220:
Coccyx [x-rays] Not routinely indicated. Normal appearances often misleading and findings do not alter management. (RCR guidelines 1998)
Page 41 of 220:
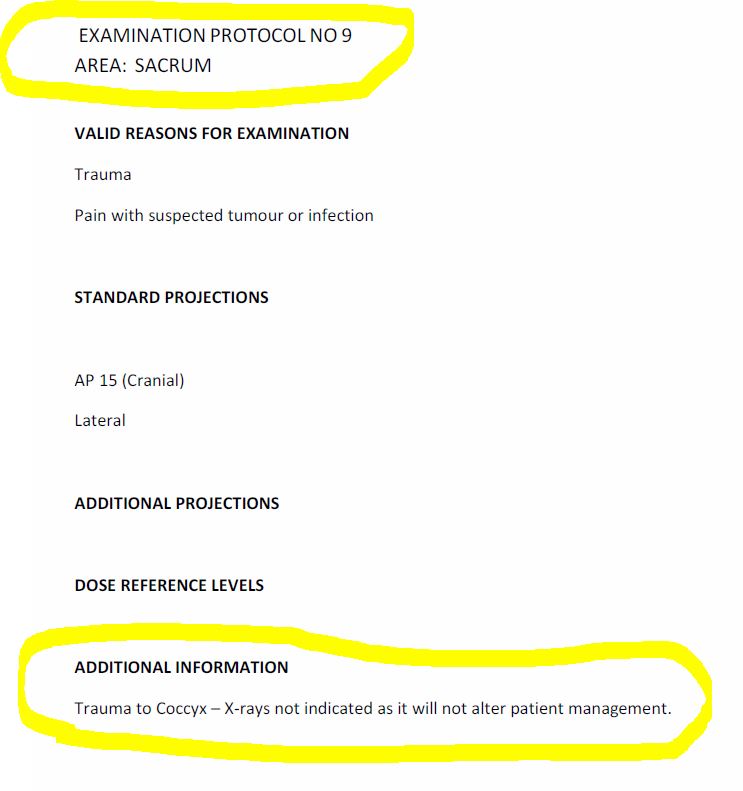
EXAMINATION PROTOCOL NO 9
AREA: SACRUM
VALID REASONS FOR EXAMINATION
Trauma
Pain with suspected tumour or infection
STANDARD PROJECTIONS
AP 15 (Cranial)
Lateral
ADDITIONAL INFORMATION Trauma to Coccyx – X-rays not indicated as it will not alter patient management.
Dr. Foye’s response:
I think that their protocol is severely misguided and shows a lack of understanding of coccyx pain and a lack of compassion for those who suffer from it.
The radiology protocols also suggest that clinicians in the UK would not know how to make useful decisions and treatment plans based on the x-ray results. The protocol is essentially implying that in the UK their medical doctors, chiropractors, physical therapists, etc., are too ignorant of how to use the x-ray results, so let’s ban the x-rays from being done in the first place. By contrast, I believe and I know that there are indeed clinicians in the UK who are well aware of how to make important treatment decisions based on the x-ray results.
In 2016, I (Dr. Foye) previously addressed a similar nihilist attitude that a radiology journal had published against the use of coccyx x-rays in hospital Emergency Departments.
To their credit, the journal published my response (here is that Link: https://www.ajronline.org/doi/abs/10.2214/AJR.16.16542), where I offered the following critiques. The point that I raised, shown below, also apply to the NHS radiology protocols:
“Did they include sacrococcygeal collimation (i.e., coned-down views to obtain clearer bony definition), which is especially important for the small coccygeal bones?
Did their sacrococcygeal imaging include sitting-versus-standing lateral radiographs, without which the researchers would be unable to diagnose coccygeal dynamic instability, which is one of the most common causes of coccyx pain?
Instead of eliminating sacrococcygeal radiographs for patients in the emergency department, perhaps we should focus on improving sacrococcygeal radiography.”
“Meanwhile, the authors suggest that the imaging results do not affect treatment. However, their own study shows that patients without positive imaging studies receive fewer analgesic medications.”
“Unaddressed issues included patients’ emotional distress from not knowing the cause of their pain or feelings of whether the treating physicians were dismissive or unbelieving of the patients’ injuries.”
“Furthermore, accurate diagnosis creates individualized treatment options, such as fluoroscopically guided injections targeting the specific site of injury or nasal calcitonin treatment of acute fracture of a coccygeal vertebral body.”
“In summary, rather than eliminating sacrococcygeal radiography, we believe clinicians should focus on improving how these studies are performed, interpreted, and acted on.”
Screen-capture from Dr. Foye’s 2016 publication on the usefulness of coccyx x-rays in patients with tailbone pain:
X-rays ARE useful for coccyx pain, tailbone pain, explained by Dr Foye, 2016 AJR
Screen-captures from the UK’s Radiology Protocol document (from the publicly-available PDF that was downloaded from the link above) are below:
NHS Cover Page, Radiology Guidelines
NHS, Radiology HEADING
NHS, Radiology Protocol Advised AGAINST Coccyx X-rays
NHS, Sacrum Radiology Protocol Advised AGAINST Coccyx X-rays
Some patients never had tailbone pain before UNTIL very soon after they underwent neck surgery (surgery at the cervical spine, such as a cervical laminectomy, cervical discectomy, cervical fusion, etc.).
There are a few reasons why someone can have tailbone pain after neck surgery:
1) Neck surgery site causing tailbone pain:
At the time of the surgery at the cervical spine, either the surgery itself or subsequent scar tissue after the surgery can cause some pulling, or traction, upon the “Dura”.
The dura is the tissue or lining that surrounds the cerebrospinal fluid within the spinal canal.
Since the lowest end of the dura is attached near the upper part of the coccyx, it is theoretically possible for traction or pulling up at the neck to cause tension down at the coccyx.
This can potentially be a cause of pain.
2) Increased sitting/reclining after surgery causing tailbone pain:
It is possible that there was an underlying coccyx condition all along, but it was not causing any symptoms.
Examples of such underlying tailbone problems include: coccyx arthritis, or coccyx bone spur, etc.
They may have never been symptomatic until the patient spent a significant amount of time laying or reclining.
Especially problematic our hospital beds, where patients often have their legs out straight but the head of the bed elevated so the patient is in a somewhat reclining position.
This position of sitting in a hospital bed or recliner puts a significant amount of pressure on to the sacrum and coccyx.
In fact, this is largely why that specific area is a common site for bedsores in hospitalized patients.
For someone with an underlying tailbone problem that never caused symptoms before, the time spent in this semi-reclined position may cause the tailbone problem to actually become painfully symptomatic.
3) Coincidence:
Sometimes, the tailbone pain may be completely unrelated to the neck surgery.
It is understandably tempting to assume that a new medical symptom that started must be related to the most recent major medical thing that happened in your life.
But sometimes two things that happen one right after the other may be completely unrelated.
Evaluation and Treatment:
Regardless of whether the tailbone pain is related to the cervical spine condition or not, it is important to have a thoughtful evaluation looking for anatomic causes of tailbone pain.
Usually, a thoughtful and thorough evaluation will reveal an underlying coccyx problem.
Common examples include coccyx arthritis, bone spurs, and probably most common is unstable joints at the tailbone.
(To evaluate for unstable joints at the tailbone, patients need to have a special type of coccyx x-rays done specifically while the patient is sitting. The coccyx x-rays are done while sitting since that is the position that is usually most painful and that is the position where the patient’s body weight is on the tailbone and may be causing abnormal movement of the coccygeal bones.)
And this is the next in a series of videos looking at the different chapters in my book “Tailbone Pain Relief Now!”
And the idea is just to give a glimpse into the general material that’s covered within the different chapters, which then provides us with an opportunity to talk about those areas and to post questions and comments down below, to have a dialogue about this.
This chapter, for this video, is Chapter number Six, which I think is perhaps the most important chapter in the book because it it’s about unstable joints of the coccyx or tailbone.
And the reason I say it’s perhaps the most important chapter is for two reasons.
Number one is that this is perhaps the most common cause of tailbone pain.
Certainly in our practice here patients fly in from around the country and internationally, and far and away the most common diagnosis that we find is that they have instability, an unstable joint or more than one unstable joint at the tailbone.
And the second reason why this is such an important topic is that this is an area that is widely under-diagnosed.
The vast majority of people who have this condition have never had the proper testing done to evaluate for it so.
So, in this chapter… again we’re looking at here Chapter 6 about the unstable tailbone, which is basically that the joints are unstable and that contributes to a condition that medically we call that instability and specifically dynamic instability which we’ll talk about.
So in this chapter… it starts off with a story of a patient, like hundreds and hundreds of patients who I have seen who have been told that there’s nothing wrong with their tailbone, that everything is fine, that the plain x-rays and even the MRI or CT scan looked okay.
But the patient failed to have a sitting versus standing x-ray done.
So, given that your pain with tailbone pain is usually worse WHILE YOU’RE SITTING, the x-rays really should be done WHILE YOU’RE SITTING.
But unfortunately very few places know about how to do those properly.
Very few radiology centers or hospitals have even heard of doing these x-rays of the tailbone while sitting.
So that means that they don’t get done.
And because they don’t get done we don’t get to see what happens to the tailbone when you’re putting your body weight on it by sitting.
When we sit, sitting down puts pressure on to the tailbone.
And the tailbone then may move or shift depending on the on the pressure that’s placed upon it while sitting.
So what can happen is the following… you can have x-rays that look totally normal while the person is standing up or laying down, they’re not putting their body weight onto the tailbone as shown in this part of the image here.
The alignment looks okay. Everything looks fine.
But then when the patient sits, the body weight pushing on that unstable joint can cause the joint to go into a partial or complete dislocation position, as shown in this part of the image here.
So this is very very common.
I would say at least 60% or more of the patients who I see for tailbone pain have instability.
They have hypermobility as another way of referring to this: “hyper” means “increased”, and “mobility” is just talking about the “motion.”
So a couple of medical terms that are saying the same thing: it might be described as “hyper- mobility” or “instability” and “coccygeal” referring to “coccyx hypermobility”, “coccygeal instability”.
It is sometimes referred to as “dynamic instability.”
The dynamic part being that the tailbone is not just dislocated, but it’s actually moving.
It’s dynamic. It’s in one position while you are standing up or laying down, and it’s in a different position when you’re putting your body weight on it by sitting (and especially if you’re sitting leaning part way back, that puts even more of your body weight and pressure onto the tailbone).
So in the chapter, Chapter Six, is really, really super important because for people who are suffering with tailbone pain if you have not had an evaluation to see if you have dynamic instability, hypermobility (again all saying the same thing here), if you have not had that evaluation done with sitting-versus-standing x-rays, then really you have not had the appropriate or adequate testing to find the cause of your tailbone pain.
So the chapter goes into a lot more of the details really the point of the video is just to give you a taste for the topic and that allows us to have more of a dialogue in the comment section down below.
For more of the details they’re certainly in here about different types of dynamic instability.
This shows one type which is where there’s what’s called listhesis or sliding.
But there are other types as well. There are patients who have a tailbone that flexes too far forward or too far backwards, which we can show that on this model.
(This model is a little worn down from over the years…)
But if you sit then the tailbone flexes or bends too far into the forward position.
Or in some patients it actually extends backwards.
Those are examples of increased mobility, or hypermobility.
Any of those can be painful because when you’re having that increased movement at the joint then you’re having extra mechanical stress and forces and pressure on the joint, which can be very painful.
Just like if my thumb was going into this kind of a dislocation, if it was shifting that much of course it would be painful.
And any doctor or clinician would understand that.
But at the tailbone unfortunately it’s a little bit “out of sight out of mind.”
Physicians are not aware of this phenomenon at the tailbone, even though they’re well aware of it in other parts of the body and throughout the rest of the spine.
So again it becomes really important to have the appropriate testing done to evaluate for that. There are specific criteria for how much movement there is supposed to be at the tailbone in terms of that sliding or movement forward and backward up to 25% of the of the width of the of the actual bone itself.
There are cut-offs also for how much the tailbone is supposed to flex forwards when you sit and put your body weight onto it.
The original sources typically say flexing forward by 20 degrees.
And again if it’s moving more than the standard normal amount, then that by definition would be hypermobility or increased mobility.
So I go into a lot of that here in terms of the different types of hypermobility and the tests that can be done, which as we mentioned is the sitting versus standing x-rays.
You do the x-rays in the side view looking from both positions: while you’re sitting and also while you’re standing. And then we compare because that comparison is really what’s important: to see how much movement there is when you go from one position to another.
So that’s the general idea.
The toughest part which is actually the last part here, which is where can you find a place that will do this sitting versus standing x-rays.
And that becomes a real challenge unfortunately for many many patients, because again most radiology departments are not familiar with this. There is information that that is available online that will help to give instructions to the radiology centers or certainly you can share with them the information that’s in the book so that that can help you to get things going in the right direction hopefully.
But admittedly I do understand it is an uphill challenge for places that are not familiar with it to convince them to do the appropriate testing.
So that’s the general the general gist.
There’s a lot more detail in here but I’m trying to keep the videos less than 10 minutes and really just to provide an opportunity then for us to discuss down in the comment section down below.
So post your comments down there and myself and others can interact and comment on the topic.
So if you have questions about sitting versus standing x-rays or hypermobility at the coccyx post your comments down below.
If you’re looking for a copy of the book, the easiest way to find that is to go to www.TailboneBook.com
and if you’re looking to find me online, or to come for evaluation here, the easiest way to find me is to go to the website www.TailboneDoctor.com
I hope that’s helpful.
Post your comments down below.
Bye-bye, now.
Here is the actual VIDEO:
Here is the screenshot thumbnail image for the video: