Those of you OUTSIDE of the United States may now obtain the book on Amazon, as Amazon is very well able to handle the costs and logistics of international shipping.
Book: “Tailbone Pain Relief Now! Causes and Treatments for Your Sore or Injured Coccyx” by Patrick Foye, M.D.
Note: as of 2017, you can get the e-book for a lower cost than the shipping/handling for the free paperback book, so the free book offer has been replaced by the e-book. You can still get the paperback book, which in late 2016 dropped to half-price. Use the links above.
You may wonder what topics I’ve covered in the 31 chapters of my new book, “Tailbone Pain Relief Now! Causes and Treatments for Your Sore or Injured Coccyx.” It may seem like a lot to have written 272 pages just about the coccyx.
So here is a list of the sections and chapters.
Chapter
Chapter Title
PART ONE
PART ONE: FINDING THE CAUSE OF YOUR TAILBONE PAIN
(Chapters 1 through 17)
1
Introduction
2
Symptoms of Tailbone Pain (Coccyx Pain)
3
Overcoming Stigma: Psychology of Tailbone Pain
4
Anatomy of Tailbone Pain
5
Causes of Tailbone Pain
6
Dynamic Instability of the Coccyx
7
Tailbone Fractures: the Broken Coccyx
8
Dislocations of the Tailbone
9
Bone Spurs of the Tailbone
10
Arthritis of the Tailbone
11
Abnormal position of the tailbone
12
Sympathetic Nervous System Pain at the Coccyx
13
Cancer Causing Tailbone Pain
14
Bone Infection Causing Tailbone Pain
15
Back and Buttock Pain
16
Medical Tests for Tailbone Pain
17
Consults with Other Medical Specialists
PART TWO
PART TWO: TREATMENTS FOR YOUR TAILBONE PAIN
(Chapters 18 through 25)
18
Treatments for Tailbone Pain: Overview
19
Avoiding Exacerbating Factors for Tailbone Pain
20
Tailbone Pain Cushions
21
Tailbone Pain Medications
22
Tailbone Manipulation
23
Tailbone Pain Exercise
24
Tailbone Pain Injections
25
Tailbone Surgery Coccygectomy
PART THREE
PART THREE: SPECIAL SITUATIONS REGARDING TAILBONE PAIN
My book publishing team thinks I’m crazy! I’ve worked well over 1,000 hours creating this book over the past 1.5 years. It’s 272 pages, 31 chapters, all about coccyx pain causes and treatments. Written for patients.
So they think I’m crazy to launch the book by giving it away for FREE!
But I know that lots of you are suffering with tailbone pain and I’m confident this book will help you to find the answers and relief that you need and deserve.
So, for a limited time, I’m giving away the first 50 books for FREE.
(Just pay shipping/handling: just a few dollars in the United States, more for international shipping.)
It can be challenging to get to the correct x-rays done in the medical testing for someone with tailbone pain (coccyx pain).
Unfortunately, it is VERY common that the x-rays failto focuson the area of pain (the coccyx).
Unfortunately, the tailbone x-rays include LOTS of other nearby anatomic regions, such as:
the thigh bones (femurs),
the hip joints at the middle of the pelvis,
the pubic bones at the front of the pelvis,
the lumbosacral spine at the lower back (the “small” of the back, up around the belt line).
In general, because of all of those structures are MUCH bigger than the coccyx the images tend to be washed out at the coccyx.
I often compare this to trying to take a photograph of my pinky fingernail.
Bad: If you took the photograph of my pinky fingernail with me holding my pinky in front of a bright window on a sunny day, the camera would adjust for the brightness outside that fills most of the photo. This would leave my pinky looking very washed out in the photo. This would make it difficult to see any significant details.
Good: Alternatively, if you took the photograph of my pinky fingernail by having the camera zoom in on just the structure that you are interested in (my fingernail) then you would get a nice, clear and detailed image of the structure that you are interested in.
Your ordering physician can specifically request that the tailbone x-rays be done using a “coned-in” technique
sometimes also called a “coned-down” technique
sometimes also called x-ray “collimation.”
Better and safer: In addition to providing a more clear and detailed image of the tailbone, the coned-in technique helps to decrease the amount of unnecessary radiation delivered to the patient.
Please post your thoughts, feedback, comments or questions below, regarding coned-in xrays for tailbone pain.
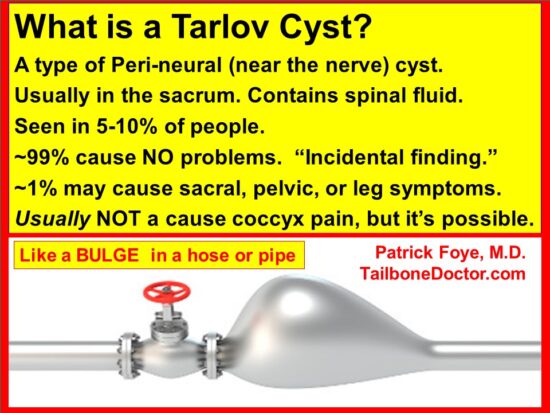
Sometimes at the sacral spine (the large bone at the back of the pelvis) there is a fluid collection known as a sacral Tarlov cyst.
I explain sacral Tarlov cysts by comparing the sacral spinal canal to a garden hose.
Have you ever seen a garden hose that gets worn down to the point where there is a bulge or out-pouching, where the wall of the hose has become worn and weak enough that the hose develops a bulge?
Now imagine that instead of a bulge filled with water from the garden hose, at the sacrum there is a bulge filled with spinal fluid from the spinal canal.
Do sacral Tarlov cysts cause pain or other symptoms?
Sacral Tarlov cysts are usually not symptomatic, but they can be.
Some dogmatic doctors will say that sacral Tarlov cysts are NEVER symptomatic, but I do not believe that is true.
Although they are USUALLY just an “incidental” finding that is noticed on MRI or CT scans, in some cases pressure from a Tarlov cyst may indeed cause symptoms.
Where do patients feel the symptoms from a sacral Tarlov cyst:
Sacral pain (pain at the back of the pelvis)
Pain down your leg or legs: If the Tarlov cyst causes pressure onto the upper sacral nerve roots, this may cause pain that down into one or both of your legs.
Pain into your pelvis: If the Tarlov cyst causes pressure onto the lower sacral nerve roots, this may cause pain that travels into your pelvis.
If the sacral nerve roots that are involved include sacral nerves 2, 3, and 4, then the symptoms may travel in the distribution of the pudendal nerve, causing pain in the distribution of that nerve (pudendal neuropathy, or pudendal neuralgia).
Pudendal nerve pain is usually a burning pain into your genital region.
Pudendal nerve problems sometimes include genital numbness, instead of pain.
Multiple different types of injections are done to decrease tailbone pain.
3 of the most common types of tailbone injections:
Steroid injection: a steroid is an anti-inflammatory medication that can be placed at a site of inflammation, to decrease the inflammation and pain at that location.
Sympathetic nerve block: Sometimes in addition to the musculoskeletal pain and inflammation there is a component of nerve pain. Performing an nerve block is when the doctor places a local anesthetic (such as lidocaine) onto specific nerves in order to temporarily shut them off. After a few hours when the nerves “wake up” again, the nerves may not be so hyper-sensitive and hyper-irritable. So the nerve pain can be dramatically decreased or even completely resolved.
Nerve ablation (destruction): if none of the other injections are helping, then one option is to intentionally destroy/kill/deaden the nerves that are carrying pain from a specific site. If the nerves can not carry pain signals from your tailbone, then the pain signals will never be sent to your brain and your quality of life may be dramatically improved.
Sequence of Injections
Steroid injection: I typically start with a local steroid injection, ideally targeting the specific area that matches the individual patient’s diagnosis. For example, if the pain seems to mainly be coming from a distal coccyx bone spur, then I would target that spot. If the pain seems to be coming mainly from a dislocated or unstable (hyper-mobile) joint then I would target that specific area. (This is why it is so important to have an accurate diagnosis firstrather than just injecting without knowing where the pain is coming from.)
Sympathetic nerve block: Depending on the response to a local corticosteroid injection, I would consider a ganglion Impar sympathetic nerve block. Sometimes I will combine the steroid injection and the ganglion Impar sympathetic nerve block (the steroid helps treat the musculoskeletal pain/inflammation while the nerve block helps treat the nerve pain).
Nerve ablation (destruction): Most patients will get good relief from either the steroid injection or the sympathetic nerve block. For those who don’t, I consider nerve ablation.
Repeating injections: If any given injection gives great relief (in terms of the amount of relief and the duration of relief) then that same injection could be repeated if the pain comes back many months or years later.
Fluoroscopic guidance:
Improved relief: In general, these injections can be done under fluoroscopic guidance so that the physician can make sure the medication is placed in the location that is most likely to relieve your tailbone pain.
Decreased risks: Fluoroscopy also helps the physician to make sure that they do not accidentally inject the medication into an area that would cause complications or side effects.
There are also other types of injections done for tailbone pain, but the 3 noted above are the most common.
Please post below any thoughts, questions, or comments you have about tailbone injections for tailbone pain.
Sometimes patients ask me whether tailbone pain (coccyx pain) can be treated by placing surgical hardware into or onto the tailbone to stabilize any instability of the tailbone.
At first consideration, this is a reasonable thought.
Firstly, unstable joints of the tailbone are one of the most common causes of tailbone pain (and this diagnosis is very frequently missed if tailbone x-rays are not done while the patient is sitting down).
Secondly, unstable joints and bones in other parts of the body are often treated by inserting a metal screw, pin, or rod, or by attaching a metal plate that spans across the unstable area in order to stabilize that location.
However, the tailbone is different than many other sites. There is no well-established surgical procedure to put hardware into or onto the coccyx to stabilize it.
But there is ONE single casewhere a surgical pin was used:
This was only tried in ONE single patient, in South Korea.
A 31 year-old woman slipped and fell onto her coccyx, causing anterior dislocation at the sacrococcygeal joint.
Surgeons put in a surgical pin:
they inserted a thin (2.4 mm diameter) wire/pin into the coccyx to treat the dislocation.
This surgery was performed VERY soon after the injury.
Specifically, it was done just eight hours after the tailbone injury.
So the surgery was done the VERY SAME DAY as the injury.
The VERY soon timing of the surgery raises multiple questions:
Would the patient’s pain have improved just as well without the surgery, just by normal, natural recovery?
What would be the criteria to justify doing surgery so soon, when data and clinical experience shows that MOST patients with tailbone injuries resolve over time WITHOUT surgery?
Would any similar surgery have any role in patients who did not have the surgery done on the same day as their injury?
Published: Joystick reduction and percutaneous pinning for an acutely anteriorly dislocated coccyx: a case report. Kim WY, et al. J Orthop Trauma. 2004.
Beware surgical cement
There was a single case report presented at a conference years ago about a doctor who injected some surgical cement into a patient’s coccyx region.
But I don’t think there was ever any follow-up after the conference in terms of how the eventual outcome was.
Also, I don’t think they ever published it as a medical journal article.
I did inherit one other/different patient who had undergone an injection of surgical cement and she reported being MUCH worse for having undergone the injection. It was sort of a mess, because now the cement blocked the areas where typical injections would be tried. Also, any surgical treatment was going to need to remove not only the focal area of the coccyx, but also was going to need to remove the extended, larger area of the cement.
If you have thoughts, comments, or experiences regarding surgical hardware at the coccyx, or regarding cement injections for tailbone pain… Please post your comments below!
Regarding complications and side-effects from coccygectomy (surgical removal of the tailbone), please click on the links below:
Colonoscopy is a medical procedure where a flexible tube is inserted into the anus and colon.
A camera on the front tip of the tubing allows the doctor to see the inside of your colon, within the large intestines.
Colonoscopy is generally considered to be a safe way of detecting abnormalities such as colon cancers.
However, any time that a medical instrument is inserted into a human body there is a risk of causing injury to the patient. I have seen multiple patients where the onset of their coccyx pain was immediately after colonoscopy.
In 2008, I published in the American Journal of Physical Medicine and Rehabilitation a case report of tailbone pain due to colonoscopy:
A woman underwent colonoscopy.
After the colonoscopy, when she awoke from sedation, she reported the new-onset of severe tailbone pain (coccyx pain, also called coccydynia or coccygodynia).
The coccydynia was felt to be have been caused by the colonoscopy, based on the positive imaging studies, the timing of the symptom onset, the lack of previous symptoms or injuries at that site, and the close proximity of the injured coccyx to the anal and rectal regions traversed by colonoscopy.
This was the first case ever documented in the medical literature where colonoscopy caused a patient to have tailbone pain.
(Reference: AJPMR 2008 Mar; 87 (3): S36)
Since then, I have seen and learned of a number of other patients whose tailbone pain either started after colonoscopy or whose tailbone pain was worsened by colonoscopy.
Conclusion: colonoscopy can now be added to the list of traumatic causes for tailbone pain.
It is not surprising that colonoscopy could cause tailbone pain.
The tailbone is very very close to the colon. The colon / large intestine is anatomically located immediately in front of the sacrum and coccyx, so it is possible that colonoscopy may cause potential trauma to the coccyx.
Pressure from the colonoscopy could push on the tailbone, especially if the tailbone anatomy is abnormal.
Probably the patients at highest risk for this are those whose tailbone is flexed too far forward, bringing it even closer to the colon.
It is also possible that pressure on the tailbone can happen AFTER the colonoscopy, while sitting in a hospital bed in recovery after the procedure.
Colonoscopy may cause or worsen tailbone pain.
And of course there are times where the coccyx pain is not related to the colonoscopy at all.
People with tailbone pain (coccyx pain) sometimes wonder…
What type of doctor treats tailbone pain?
The answer probably depends on where you are within your spectrum of treatment…
If you have mild tailbone pain of recent onset, probably your primary physician can handle this adequately by recommending a cushion and pain medications by mouth.
If your tailbone pain has been present for more than a month, or if you are not getting enough relief from the initial treatment provided by your primary medical doctor, then you should see a doctor who specializes in pain management. Ideally it should be a pain physician who has experience in treating tailbone pain.
Pain management doctors can provide pain medications given by local injection.
Pain management physicians are usually subspecialists from the fields of either 1) Physical Medicine and Rehabilitation [PM&R], or 2) Anesthesiology.
If you have pain throughout the pelvic floor, it may be very helpful to receive an evaluation and treatment from a pelvic floor physical therapist.
If your pain has been present for more than two month, or if are not getting good relief from your local clinicians, you should consider seeing a doctor who specializes specifically in coccyx pain.
This way you can get sitting-versus-standing coccyx x-rays and other expert-level evaluations to find the cause of your pain and to provide the best available treatments.
For patients who have not gotten adequate relief from medications by mouth or medications by local injection, then one consideration is surgical removal of the tailbone (coccygectomy). This is typically done by an orthopedic surgeon or specifically by a spine surgeon. Coccygectomy is necessary in less than 5% of people with tailbone pain.
Regardless of what type of doctor you are considering seeing, perhaps the most important question is whether or not the doctor has substantial experience and expertise in treating tailbone pain.
Here are 3 ways to tell if your doctor is experienced at evaluating and treating tailbone pain:
Look at the website for the doctor or their medical practice. If the website fails to mention coccyx pain, tailbone pain, or coccydynia, then clearly the doctor does not consider that to be a significant part of their medical practice.
Call the doctor’s office and ask the receptionist “Does Dr. _____ treat coccydynia?” Coccydynia is the medical term for tailbone pain. If the receptionist sounds confused, or needs you to spell or explain what coccydynia is, then clearly tailbone pain is not a common issue for patients treated in that practice. The receptionist’s job is to answer the phones all day for incoming patients and follow-up patients, and to book their appointments, hundreds of times per month. So if the receptionist has not heard of coccydynia, or has to check with someone else to find out if that practice treats this condition, then you already know the answer that usually they do not.
Ask the doctor’s receptionist whether their office provides seated coccyx x-rays (x-rays of the coccyx, done while you are sitting, since that is typically the most painful position for most people with tailbone pain). If the receptionist sounds confused, or needs you to explain what seated coccyx x-rays are, then clearly tailbone pain is not a common issue for patients treated in that practice.
Asks the doctor, “How many patients with tailbone pain have you treated in the past month?” If the doctor is not regularly treating patients with your condition, then he or she will probably be less experienced at providing the optimal testing and treatment for this condition.
As a rehab medicine physician, let me start by saying that in general… I am a big fan and a big advocate for physical therapy as a non-surgical approach to manymusculoskeletal/pain disorders.
For pelvic floor pain and dysfunction, there are a growing number of physical therapists who specialize in treating pelvic floor pain.
A pelvic floor P.T. can often be extremely helpful with a variety of conditions including some forms of:
urinary incontinence,
pelvic floor sagging/prolapse,
vaginal muscle pain during sexual intercourse,
various pelvic floor muscle spasms, tightness, etc. (including pelvic floor muscle spasms that may occur as a guarding/reactive response because of tailbone pain),
and much more!
Having said that, when it comes to focal tailbone pain the benefit (or lack thereof) of any given treatment probably depends most on the underlying cause or condition. There are some tailbone conditions that I would NOT expect P.T. (or other attempts to do mobilization of the coccyx) to be particularly helpful for:
Bone Spurs:
If the tailbone pain is being caused by a focal bone spur (which commonly occurs at the lowest tip of the tailbone) and if it is NOT associated with any muscle/tendon pain within the pelvic floor, then P.T. would probably NOT be likely to provide substantial relief.
Recent bone fractures:
if the bones of the coccyx have recently been broken (fractured), then those bones may need relative rest and a chance for the fractures to heal. As with other body regions, aggressive physical therapy too soon after fracture would have the potential to delay fracture healing.
Unstable or excessively mobile tailbone joints:
If “coccyx mobilization” is the proposed treatment, then it makes sense to wonder when that might be helpful and when that might be harmful.
Mobilization (or “manipulation”) is done to increase the movement of a joint or body region that is felt to be “stuck” or “too stiff”.
At the tailbone, mobilization is done by the clinician inserting one or two of their fingers into the anus and rectum (in front of the coccyx) while the thumb is placed in back of the coccyx. Then the clinician attempts to move (mobilize) the tailbone.
However, if the tailbone is already moving too much (due to unstable joints causing excessive mobility) then mobilizing the tailbone might actually WORSEN the problem.
This is important since probably the MAJORITY of patients with tailbone pain have undiagnosed joint instability at the coccyx.
So this MAJORITY of patients would have a condition for which we would typically recommend AGAINST attempting additional mobilization.
In the comments section below, I would love to hear from:
Any pelvic floor physical therapists who have input on pelvic floor PT specifically for patients with tailbone pain. Feel free to agree, disagree, or just add additional perspectives and dialogue regarding this challenging area.
Any people with tailbone pain who have tried pelvic floor PT. What were the biggest benefits? What were the biggest limitations? Any other thoughts… ?