Coccygectomy is surgical removal of the tailbone (essentially amputating the tailbone).
There are not great long-term studies about long-term complications of having the tailbone removed.
The short-term risks include infection at the surgical site, especially in the first few weeks or months after the surgery.
Infection: In some studies up to 20% of patients need to have repeat/additional surgery to remove the infected tissue, and the infection rate is generally figured to be due to the tailbone being so close to the anus and therefore the surgical site really cannot be sterile the way that other body regions can be.
Longer-term risks include persistent pain and pelvic floor prolapse.
Persistent pain: unfortunately, although coccygectomy is usually effective at removing some of the patient’s tailbone pain, usually the relief is not complete. It is very common that some pain will persist.
Pelvic floor prolapse: Some of the pelvic floor muscle/tendon/ligaments do indeed attached to the coccyx, and certainly there have been case reports of people who have suffered from “pelvic floor prolapse” after coccygectomy, which is sagging of the pelvic floor.
Regarding complications and side-effects from coccygectomy (surgical removal of the tailbone), please click on the links below:
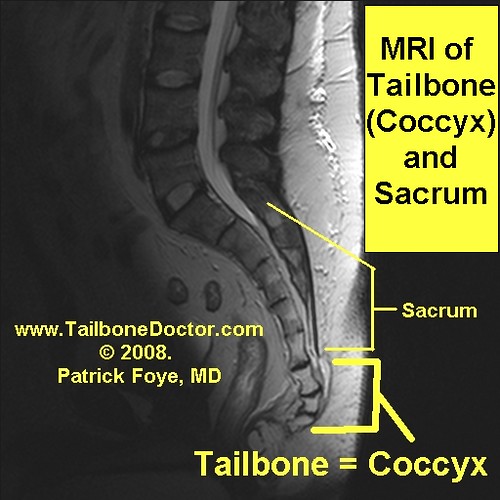
If you had an MRI done for your tailbone pain (coccyx pain, coccydynia) you should try to get a copy of the computer CD containing your MRI images.
Ideally you should review the actual images with your treating physician (typically the physician who ordered the MRI). It’s a very bad sign about your treating/ordering physician if they are not willing or able to review your tailbone MRI images with you.
But if the MRI facility gave the CD directly to you, you may be interested to check it out yourself, even prior to bringing it to your doctor’s visit. Read below for tips on how to view your CD at home.
Here are some typical steps to open and view your MRI images on your own computer:
Typically when you load the computer CD in your computer the CD will open up and show a bunch of different files and folders.
If on your computer you have your folder display options set to “show details”, then it will show you not only the electronic file names for those files/folders but also the details about what types of files they are.
Usually there will only be one file that is classified as an “application” file.
Typically, if you click or double-click on that specific “application file” it will run the program that will show the images.
It may take a minute or two to load the program and bring up the program’s control panel.
Directions get trickier after that because every different MRI manufacturer has different software, so different ones use different control buttons for scrolling through the hundreds of images associated with a single MRI study.
For example, sometimes you need to double-click on a batch of images to display them.
Other programs require you to click on a batch of images and drag/drop them onto a display field.
Some programs will have you use the arrow buttons on your keyboard to advance from one image to the next, or from one group of images to the next.
Other programs will have you use the “page up” or “page down” button on your keyboard to do this.
Still others will require you to use your mouse to click on an icon up in the toolbar to do this.
Similarly, there will be control buttons to click on (or keyboard shortcuts) for your to look at further details of the images by making the image more or less bright, or adjusting the contrast up and down, or zooming in on an area of question/concern. Again, the details for how to do this varies from manufacturer to manufacturer.
Take a photo: If you see something interesting or concerning on your computer screen, or anything that you just have a general question about, you may want to take a photo of it using your smartphone, so that you can show it to your doctor in case he/she has trouble opening the CD in their own office. When you are taking a smart phone/iPhone photo of your computer screen, you may want to turn off the lights in the room (to minimize reflection/glare).
A “bone scan” is a test performed by the nuclear medicine part of a radiology center.
A “Nuclear Medicine Bone Scan” is generally considered to be very good for detecting bone destruction from things like bone cancer (malignancy), bone infection (osteomyelitis), or bone injuries (such as fractures).
If the bone scan is truly being done to look for tailbone pain (coccyx pain), you must make sure that the bone scan actually includes the tailbone (coccyx)!
Many doctors are not aware that a standard Nuclear Medicine Bone Scan does NOT include views of the tailbone.
In the standard way that a Nuclear Medicine Bone Scan is done, the images are done with a view from the front or the back, but not with a view from the side. Those standard front or back images unfortunately cause the view of the tailbone and lower sacrum to be BLOCKED (obstructed) by the nuclear medicine material in the urinary bladder at the front of the pelvis.
(Bone scans use nuclear medicine material that lights up bony fractures, tumors, etc. This nuclear medicine material is given intravenously through the IV, then filtered by the kidneys and it collects in the urine within the urinary bladder at the front of the pelvis, where it typically blocks the view of the tailbone. It’s sort of like the nuclear material in the urinary bladder causes a “shadow” blocking out the ability to see what is going on at the tailbone. )
Thus, the standard technique for a Nuclear Medicine Bone Scan will show a clear picture of ESSENTIALLY the entire body… EXCEPT for the coccyx and lower sacrum.
Thus, the doctor may order the Nuclear Medicine Bone Scan to check for a cancer at the sacrum or coccyx, but then the test will show essentially the entire body EXCEPT for the area that the patient and doctor are interested in!!
I have unfortunately seen MANY patients who previously had a bone scan done were tailbone problems, only to be told that it was normal, and then many months later when they come for a consult with me we realize that the bone scan never even included any views showing the tailbone at all!! It’s absolutely crazy, but it happens very often.
The result is that the doctor and patient think that a Nuclear Medicine Bone Scan has done a good job of making sure there was no cancer or infection at the coccyx, when in reality the bone scan failed to look at that area. So maybe there actually is a cancer or infection there but the Nuclear Medicine Bone Scan missed it.
The way to avoid this problem is for the doctor to explicitly order the Nuclear Medicine Bone Scan to include images of the pelvis/sacrum/coccyx FROM THE SIDE VIEW, instead of just the front and back views.
The medical phrase for this side view is a “lateral view”.
The doctor and patient can explicitly request that the radiology center include side-views (lateral views).
If you already had a Nuclear Medicine Bone Scan done, then there are some important steps to take…
Obtain a paper copy of the Nuclear Medicine Bone Scan official, typed radiology report. Read the report and confirm whether the radiologist actually commented explicitly on the appearance of the tailbone. Look for the words coccyx, coccygeal, or sacrococcygeal. If the report fails to specifically mention the appearance of the coccyx, coccygeal, or sacrococcygeal areas, then there is a high likelihood that those areas were not properly seen or included in the images that were done.
Also obtain an electronic copy of the actual bone scan images (typically on a computer CD) and ask your treating physician to specifically point to the tailbone on the images. Often, the doctor will be surprised to realize that the tailbone was not included at all!
Ryan Villopoto recently retired from his motocross (motorcycle racing) career due to an April 2015 crash in Italy that reportedly caused multiple tailbone fractures (broken bones of the coccyx) and low back injuries of the lumbar spine.
Villopoto is only 26 years old, but was already an accomplished motorcycle racer, including six-time Motocross champion, four-time Supercross champ, and winner in the 250 class in 2007 at Spring Creek.
Motocross champion Ryan Villopoto. Source: “Ryan Villopoto MXoN 2008” by Mark – Flickr: Red Bull FIM Motocross of Nations 2008. Licensed under CC BY 2.0 via Wikimedia Commons – https://commons.wikimedia.org/wiki/File:Ryan_Villopoto_MXoN_2008.jpg#/media/File:Ryan_Villopoto_MXoN_2008.jpg
A United States military veteran with tailbone pain (also called coccyx pain, or coccydynia) turned out to have cancer and infection (a pus-filled abscess) in the tailbone region.
This shows the importance of proper medical care and thorough medical work-up.
Surgical removal of the tailbone (coccyx) is medically known as coccygectomy.
In the United States the coccygectomy surgery would often be considered an outpatient surgery, meaning that you have the surgery in the morning and go home by that evening. But that may vary depending on how someone is doing in the recovery area after the surgery, etc.
Different surgeons use different approaches for handling the fluid drainage from the surgical site. Some surgeons will send the patient home with a drain in place. The drain lets fluid flow out from the surgical site so that it does not form a big collection at the site.
The rate of infection at the surgical site is unfortunately much much higher than it is for most other elective surgical procedures. So many surgeons doing tailbone removal surgery (coccygectomy) give the patient antibiotics even before there is any infection, to prevent an infection from taking hold. There is high variability on the details of how many doses to give and which antibiotics to use.
Regarding complications and side-effects from coccygectomy (surgical removal of the tailbone), please click on the links below:
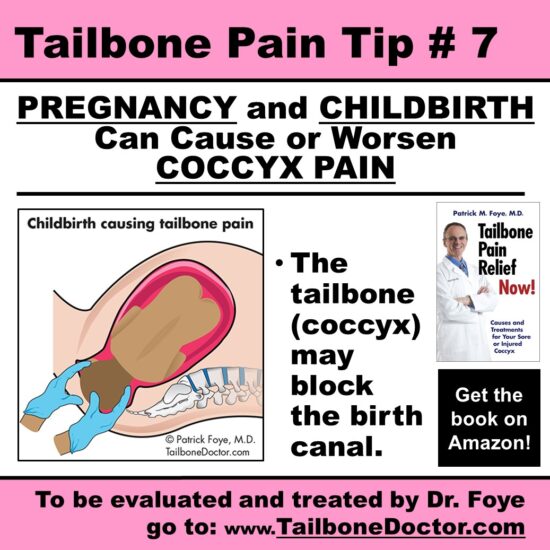
I have treated many women whose tailbone pain began during pregnancy or while giving birth (during labor and delivery).
Some of these women ask me what they should do if they are considering another pregnancy.
I sometimes advise those patients to speak with their obstetricians/gynecologists regarding considering C-section for their next pregnancy. A cesarean section (C-section) delivers the baby through a surgical incision at the lower abdomen. This way, the baby does not need to pass through the pelvic birth canal.
The rationale for considering a C-section is that a repeat vaginal birth would probably exacerbate the woman’s coccydynia.
I would not be so dogmatic to say that any subsequent childbirth/delivery should ONLY be via C-section. But, I would say that delivery by C-section would be medically indicated and reasonable in hopes of minimizing the chance of childbirth/delivery-related worsening of her coccyx pain.
This is especially worth considering in cases where prior onset of coccyx pain was via childbirth/delivery.
Another factor is whether the woman has persistent anatomic abnormalities (such as unstable joint of the tailbone, diagnosed by sitting/seated x-rays of the tailbone).
Unstable joint of the tailbone may become worse during the increased ligament laxity (looseness of the ligaments) during later pregnancy.
Also, during labor/delivery the woman should avoid prolonged coccyx pressure (which often happens to a woman who spends significant time in the semi-reclined position during labor).
Tailbone Pain Tip 7, PREGNANCY and CHILDBIRTH Can Cause or Worsen COCCYX PAIN, Tailbone Pain, Coccydynia
COME FOR RELIEF: For more information on coccyx pain, or to be evaluated in-person by Dr. Foye’s Coccyx Pain Center in the United States, go to: www.TailboneDoctor.com
– Patrick Foye, M.D., Director of the Tailbone Pain Center, New Jersey, United States.
One complication of surgical tailbone removal (coccygectomy) is that infection may occur at the surgical site.
Part of the reason for the relatively high likelihood of infection at this surgical site (compared with others) is that the coccygectomy site is so close to the anus.
Superficial infections can happen at the skin, which is called cellulitis.
Much more problematic are deep infections within the remaining bones. Bone infection is called osteomyelitis. When there is an infection within the bone, this can sometimes smolder in the background, unrecognized for many weeks or multiple months. Because the bone is deeper than the skin, it may not be immediately obvious that there is an infection.
Symptoms may include persistent or recurrent fevers, chills, ongoing pain at the site of the bone infection.
Blood work: Medical tests for tailbone infections may include blood work, looking for:
elevated white blood cells,
elevated erythrocyte sedimentation rate [ESR],
elevated CRP,
etc.
Imaging studies: Medical tests for tailbone infections may also include imaging studies, such as:
x-rays,
MRI,
CT scans,
nuclear medicine bone scans,
etc.
Treatment typically includes a much more aggressive course of antibiotics, such as:
giving the antibiotics intravenously (IV),(instead of by mouth)
and giving these antibiotics for several weeks instead of just for several days.
Regarding complications and side-effects from coccygectomy (surgical removal of the tailbone), please click on the links below:
Many patients ask me what to do about tailbone pain that continues or returns despite the person having undergone surgical removal of the tailbone (coccygectomy).
Find the CAUSE of the ongoing tailbone pain after coccygectomy
In general, it is important for the treating physician to start by searching for an underlying cause for the current pain.
Imaging studies:
Often I find that despite many months and years of pain the treating physicians have failed to order any imaging studies of the surgical site.
This would be extremely uncommon in the other body regions. If someone had severe persistent or recurrent pain despite surgery at their lower back, shoulder, knee, etc., typically the treating physicians would obtain current, up-to-date imaging studies to try to find the cause of the pain.
Did the surgery address the specific problem?
Sometimes the pain may be caused by the surgery having failed to address the actual problem that was causing the pain in the first place. For example, perhaps the pain was being caused by an unstable joint at the upper part of the coccyx, but the surgery only removed the lower part of the coccyx. In that case, the problematic joint still remains, and so it continues to cause painful problems.
Or, perhaps a new problem has occurred. For example, sometimes there might be a bone infection (osteomyelitis) at the surgical site.